Basal cell carcinoma, or BCC, is the most frequently diagnosed cancer in the United Kingdom. For many patients it is also the first encounter they have with the word "cancer" on their own medical notes — and understandably, that can feel frightening. The reassuring truth is that BCC is almost always curable when treated appropriately, and the overwhelming majority of patients I look after return to normal life within a few short weeks.
This guide sets out what BCC actually is, how to recognise it, and what you can realistically expect from diagnosis, treatment and recovery.
What is basal cell carcinoma?
BCCs arise from the basal layer of the epidermis — the deepest row of cells in the outermost layer of skin. They grow slowly over months or years and, unlike melanoma, they rarely spread to other parts of the body. What they can do, however, is burrow locally: a neglected BCC on the nose or around the eye can cause significant tissue destruction if left untreated. That is why early recognition and removal matter.
BCC accounts for roughly three in four non-melanoma skin cancers diagnosed in the UK. It is most often seen on sun-exposed sites, with the face, scalp, ears, neck, shoulders and backs of the hands being the most common.
How BCC can appear
There is no single "look" for a BCC. Several subtypes behave differently and need different treatments, which is why a biopsy is so valuable before planning surgery.
- Nodular BCC: the classic presentation — a pearly, translucent bump, often with fine blood vessels visible on the surface. It can ulcerate centrally and leave a scabbing sore that never quite heals.
- Superficial BCC: a pink, slightly scaly patch with a thin rolled edge, frequently on the trunk or shoulders. Easily mistaken for eczema or a stubborn patch of dry skin.
- Pigmented BCC: contains brown or black pigment and can masquerade as a mole or even melanoma. More common in people with darker skin tones.
- Morphoeic (sclerosing) BCC: a firm, scar-like patch with poorly defined edges. This subtype extends further than it appears on the surface and is more likely to need Mohs surgery.
Who is at risk?
BCC is ultimately a disease of cumulative ultraviolet exposure, but several factors tip the balance.
- Fair skin, light eyes and light hair: skin that burns easily and tans poorly carries the highest risk.
- Lifetime UV (Ultraviolet) exposure: outdoor occupations, recreational sun exposure and sunbed use all contribute.
- Age: incidence rises sharply after the age of 50, although younger patients are now presenting more often.
- Immunosuppression: transplant recipients and patients on long-term immunosuppressive medication face a substantially increased risk.
- Previous skin cancer: a single BCC is the strongest predictor of another — around 40% of patients develop a second BCC within five years.
- Previous radiotherapy or chronic inflammation at a particular site.
"If you have had one basal cell carcinoma, you are not unlucky — you are in a higher-risk category. Annual skin review for the rest of your life is one of the kindest things you can do for yourself."
How BCC is diagnosed
Diagnosis usually begins with dermoscopy — a magnified, polarised examination of the lesion that reveals patterns invisible to the naked eye. Where the diagnosis is in any doubt, or where planning detailed surgery would benefit from a tissue sample, a small punch or shave biopsy is performed under local anaesthetic. Results typically return within one to two weeks and confirm both the diagnosis and the subtype, which guides treatment choice.
Treatment options
The right treatment depends on the subtype of BCC, its size and location, and the patient's general health. In most cases, surgical removal offers both the highest cure rate and the best cosmetic result.
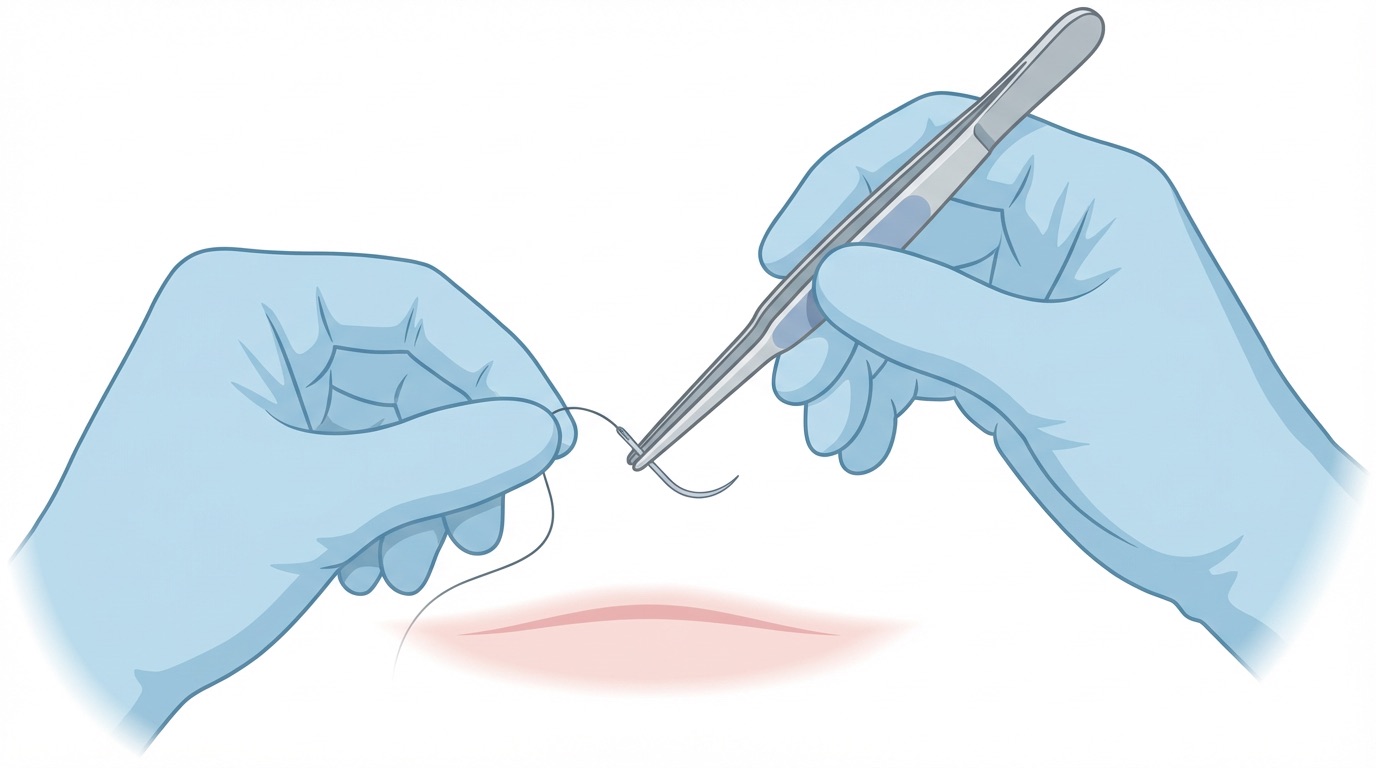
Surgical excision
This is the first-line treatment for the majority of BCCs. The lesion is removed under local anaesthetic along with a margin of healthy skin, and the defect closed directly or with a small local flap. Cure rates exceed 95% for well-defined, low-risk lesions.
Mohs micrographic surgery
Mohs is a specialist technique reserved for high-risk BCCs — particularly those on the central face, recurrent tumours, morphoeic subtypes or lesions with poorly defined edges. A dermatological surgeon removes the cancer in thin layers and checks each under the microscope in real time, so no cancer is left behind and no healthy tissue is sacrificed unnecessarily. As a plastic surgeon I frequently reconstruct the defects left after Mohs, often on the same day.
Topical treatments
For selected superficial BCCs, creams such as imiquimod or 5-fluorouracil applied over several weeks can give good results. Photodynamic therapy — a light-activated treatment — is another non-surgical option in carefully chosen cases.
Radiotherapy
Radiotherapy has a well-established role in patients who are unfit for surgery, in particular anatomical sites, or where surgery would leave an unacceptable cosmetic result. Treatment is delivered over several short sessions and is usually very well tolerated.
Recovery after surgery
Most BCC excisions are straightforward day-case procedures. You can expect the following in the days and weeks that follow:
- First 48 hours: a simple dressing, mild tenderness, and a few paracetamol-level aches at most.
- First two weeks: sutures removed at 7 to 14 days depending on the site. Bruising and a pink, firm scar are entirely normal.
- Six to twelve weeks: the scar gradually softens and fades. Silicone gel, scar massage and strict sun protection all help.
- Twelve months: final scar appearance — in most cases a thin, pale line that is far less noticeable than patients expect.
Surveillance after treatment
Because the strongest predictor of a future skin cancer is a previous one, lifetime surveillance is recommended after a BCC. In practice this usually means an annual whole-body skin examination, combined with confident self-examination at home. I encourage patients to photograph any areas of concern between appointments and to bring those images to clinic.
If you would like a baseline skin assessment, or if a lesion is behaving in a way that concerns you, the Skin Cancer Centre offers rapid access to dermoscopy, biopsy and definitive treatment. For an overview of warning signs, you may also find our article on early signs of skin cancer helpful.