Sentinel Lymph Node Biopsy
Sentinel lymph node biopsy (SLNB) is a minimally invasive staging procedure used most commonly in patients with melanoma. It identifies and examines the first lymph node (or nodes) to which a skin cancer would be likely to spread, providing crucial information to guide further treatment and prognosis.
Overview
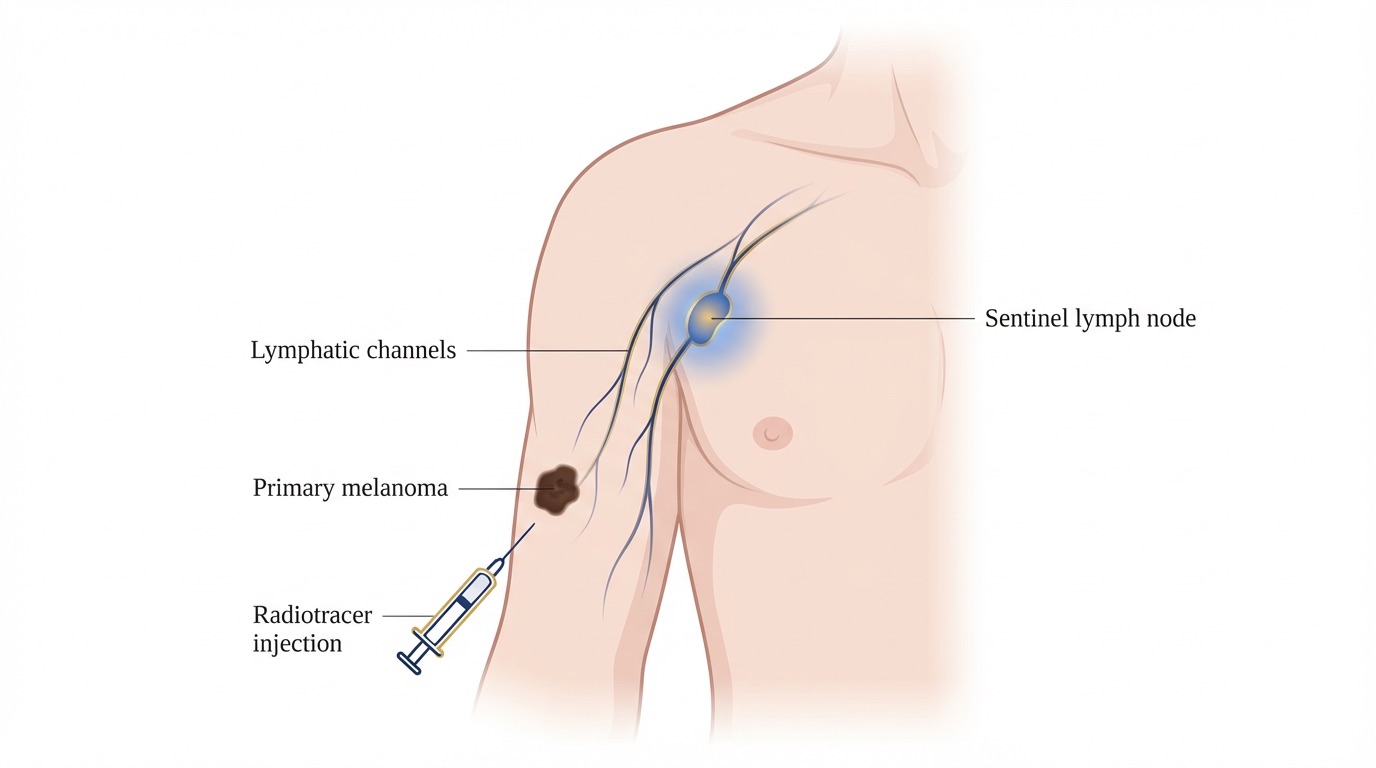
The lymphatic system drains fluid from the skin through a network of channels that reach regional lymph node basins such as those in the groin, armpit or neck. When cancer cells from a melanoma spread, they typically travel through this lymphatic system and lodge first in one or two specific “sentinel” nodes before involving others. Identifying and examining these nodes allows the pathologist to detect microscopic disease that would not be visible on scans or clinical examination.
Sentinel lymph node biopsy is recommended for patients with melanomas above a certain Breslow thickness or with other high-risk features, in line with national and international guidelines. The procedure is carried out under general anaesthetic at the same time as the wider local excision of the melanoma scar.
Benefits
- Accurate staging: Provides the most accurate information about whether microscopic cancer cells have spread to the regional lymph nodes.
- Prognostic information: The result is one of the most important predictors of long-term outcome and helps guide further treatment.
- Access to additional treatments: A positive result may make you eligible for adjuvant systemic therapies such as immunotherapy, which can significantly reduce the risk of recurrence.
- Minimally invasive: Only one or a small number of nodes are removed, rather than the entire nodal basin, minimising morbidity.
- Combined procedure: Usually performed at the same time as the wider excision of the primary tumour site, avoiding the need for a separate operation.
- Guides surveillance: The result helps to tailor the intensity and type of follow-up and surveillance imaging.
Surgical Techniques
Sentinel lymph node biopsy combines nuclear medicine imaging with a surgical dissection technique, enabling precise identification of the sentinel nodes on the day of surgery.
- Radiotracer injection (lymphoscintigraphy): On the morning of surgery, or sometimes the day before, a small amount of radioactive tracer is injected into the skin around the melanoma scar. The tracer drains along the lymphatic channels to the sentinel nodes, which are then identified on nuclear medicine scans and marked on the skin.
- Blue dye injection: In the operating theatre, once the patient is under general anaesthetic, a small volume of blue dye is injected around the scar. The dye travels along the same lymphatic pathway and visibly stains the sentinel nodes blue.
- Gamma probe localisation: A handheld gamma probe is used intra-operatively to detect the radioactive signal from the sentinel nodes, allowing a small incision to be made directly over them.
- Node removal: Any node that is blue, radioactive (hot) or clinically suspicious is carefully dissected free and removed. Usually 1 to 3 nodes are taken in total.
- Wider local excision: At the same time, the scar from the original melanoma biopsy is excised more widely with an appropriate margin based on the Breslow thickness.
- Closure: The wounds are closed in layers with absorbable sutures. A small dressing is applied and a drain is rarely needed.
Risks & Considerations
General Risks
- Infection: A small risk of wound infection which may require antibiotics.
- Bleeding: Minor bleeding and bruising are common; a haematoma occasionally requires drainage.
- Scarring: Small scars are left at both the primary excision site and the lymph node basin.
- Anaesthetic risks: Standard risks associated with general anaesthesia apply.
Specific Risks to Sentinel Lymph Node Biopsy
- Seroma: A collection of lymphatic fluid can develop at the biopsy site and may require aspiration, sometimes more than once.
- Lymphoedema: A small risk of long-term swelling of the limb draining to the affected node basin, although this is much less common than after full lymph node dissection.
- Nerve injury: Small sensory nerves near the node can be stretched or divided, leading to a patch of numbness; rarely, larger nerves (such as branches of the facial or accessory nerves) may be affected.
- Blue dye reactions: Temporary blue staining of the skin at the injection site and blue or green urine for 24 to 48 hours; rare allergic reactions can occur.
- False-negative result: Rarely, microscopic disease can be missed if the true sentinel node is not identified or removed.
- Need for further surgery: A positive sentinel node used to mean a completion lymph node dissection; current guidelines more often recommend close surveillance or systemic treatment, but further surgery may still be appropriate in some cases.
Recovery
Wound Care
- Dressings: Waterproof dressings are usually applied and can be kept in place for several days; gentle showering is permitted from 48 hours.
- Cleaning: Once the dressings are removed, gentle washing with mild soap and water is encouraged and the wounds should be dried carefully.
- Sutures: Absorbable sutures are usually used and do not need to be removed.
- Activity: Light activity can be resumed within a few days; heavy lifting, vigorous exercise and swimming should be avoided for 2 to 3 weeks to reduce the risk of seroma and to allow wounds to heal.
Scar Advice
- Scar Care Products: Silicone gels or sheets and regular moisturising help optimise the appearance of scars once the wounds are fully healed.
- Sun Protection: Protect all scars from direct sun for the first 6–8 weeks to minimise pigmentation changes, and maintain good sun protection for the rest of your skin to reduce the risk of further skin cancers.
- Massage: Once the wound is fully healed, gentle scar massage can help soften and flatten the scars.
Follow-Up
- Initial Post-Op Visit: A wound check is typically arranged around a week following surgery.
- Histology & MDT: The sentinel nodes are examined in detail by the pathologist and the results are discussed at the skin cancer multidisciplinary team meeting, usually within 2 to 3 weeks. You will be contacted with the result and any recommended next steps.
- Surveillance: Ongoing melanoma surveillance is arranged in line with national guidance, including regular clinical examinations and, where appropriate, surveillance imaging.
- Self-Examination: You will be advised on how to examine your skin and lymph node areas and when to seek urgent review.
- Long-Term Care: Mr Singh remains available for any concerns or further follow-up as required throughout your surveillance period.
Procedure Summary
Ready to Discuss Sentinel Lymph Node Biopsy?
If you have been diagnosed with melanoma and would like to discuss whether sentinel lymph node biopsy is appropriate for you, please feel free to contact us to answer any questions you may have or to schedule a consultation with Mr Singh.
Book a Consultation