Lymph Node Dissection
Lymph node dissection, also known as lymphadenectomy, is the surgical removal of all the lymph nodes within a regional nodal basin. It is most commonly performed in the management of melanoma and other skin cancers when there is clinical or radiological evidence of lymph node involvement, with the aim of controlling disease in the nodal basin and supporting further systemic treatment.
Overview
Regional lymph nodes are grouped in predictable anatomical basins including the neck (cervical and parotid), axilla (armpit) and groin (inguinal and ilio-obturator). Skin cancers such as melanoma and high-risk squamous cell carcinoma can spread through the lymphatic channels to these nodes. When enlarged nodes contain cancer cells that have been confirmed on biopsy or imaging, removal of the whole nodal basin, known as a therapeutic or completion lymph node dissection, may be recommended.
The goal of lymph node dissection is to achieve local disease control in the nodal basin, provide detailed pathological staging, and form part of a broader treatment plan that may also include immunotherapy or radiotherapy. Mr Singh carries out dissections of the axilla, groin and neck as part of a skin cancer multidisciplinary team, with the operation tailored to the basin involved and your individual circumstances.
Benefits
- Regional disease control: Removal of all involved nodes significantly reduces the risk of further disease progression within the affected basin.
- Detailed staging: Examination of all the nodes provides the most complete pathological assessment of the extent of nodal involvement.
- Guides further treatment: The detailed pathology helps to determine whether additional treatments such as immunotherapy, targeted therapy or radiotherapy are appropriate.
- Symptom relief: Removing bulky, symptomatic lymph node disease can relieve pain, pressure and other local symptoms.
- Multidisciplinary care: The operation is part of a wider plan developed in a specialist skin cancer MDT to offer the best possible outcome.
- Longer-term follow-up: Patients who undergo lymph node dissection are closely monitored, supporting early detection of any further disease.
Surgical Techniques
The surgical approach depends on which lymph node basin is being dissected and the extent of disease, and is always performed under general anaesthetic.
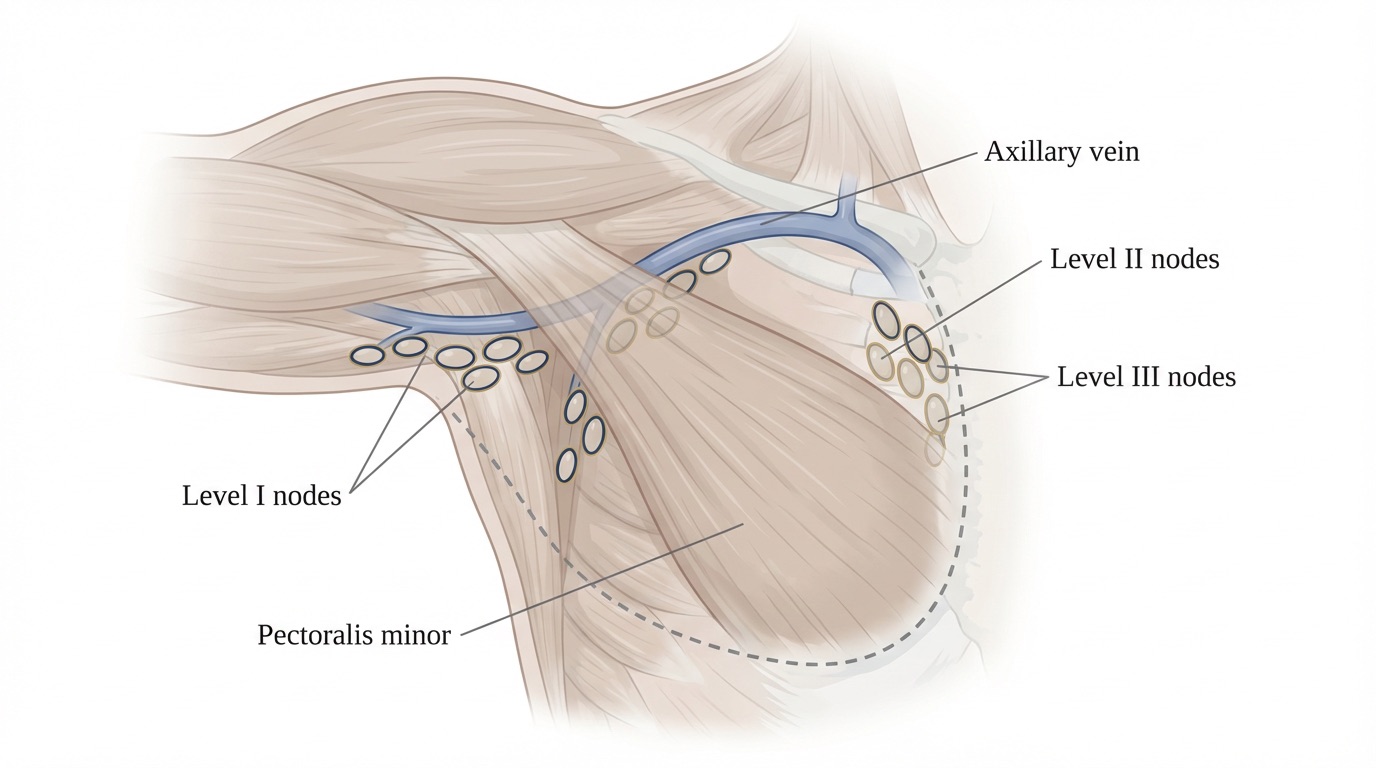
- Axillary (armpit) dissection: An incision is made in the armpit and the lymphatic tissue is carefully cleared from around the axillary vein, preserving the important nerves to the chest wall and shoulder muscles (long thoracic, thoracodorsal and medial pectoral nerves) wherever possible.
- Inguinal (groin) dissection: An incision is made over the groin and the superficial and, where indicated, deep (ilio-obturator) lymph nodes are removed en bloc, taking care to preserve the femoral vessels and femoral nerve.
- Cervical (neck) dissection: Modified or selective neck dissections remove the relevant levels of neck lymph nodes whilst preserving important structures such as the accessory nerve, internal jugular vein and sternocleidomastoid muscle whenever oncologically safe.
- Parotid surgery: When the parotid gland contains metastatic nodes, a superficial (or occasionally total) parotidectomy is performed with careful preservation of the facial nerve.
- Use of drains: One or more closed-suction drains are placed at the end of surgery to remove lymphatic fluid and reduce the risk of seroma. Drains typically stay in for several days.
- Closure and compression: The wound is closed in layers and a supportive dressing applied. Compression garments are sometimes used, particularly following groin dissection.
Risks & Considerations
General Risks
- Infection: Wound infection is relatively common after groin dissection and may require antibiotics and wound care.
- Bleeding: Bleeding or haematoma formation can occasionally require return to theatre.
- Scarring: A permanent scar is inevitable; it will be planned to lie in natural creases where possible.
- Anaesthetic risks: Standard risks associated with general anaesthesia apply, including a low risk of chest infection and venous thromboembolism.
Specific Risks to Lymph Node Dissection
- Lymphoedema: Chronic swelling of the arm (after axillary dissection) or leg (after groin dissection) is one of the most important risks. It can vary from mild to severe and may require specialist lymphoedema therapy, compression garments and long-term management.
- Seroma: Collection of lymphatic fluid in the wound is common and often requires repeated drainage after the surgical drains have been removed.
- Wound breakdown: Particularly after groin dissection, part of the wound may open and require dressings to heal by secondary intention.
- Nerve injury: Small or larger nerves in the area may be stretched, bruised or divided, leading to numbness, altered sensation or, occasionally, muscle weakness (for example of the shoulder after axillary or neck dissection).
- Numbness: Long-term patches of numbness in the inner upper arm, groin or neck are common as small sensory nerves are inevitably divided during dissection.
- Recurrence: Despite complete dissection, disease can recur within the nodal basin or elsewhere and ongoing surveillance is essential.
Recovery
Drains and Garments
- Drains: Surgical drains remain in place until the output falls below a set level, usually for 5 to 14 days. You will be taught how to manage and record the drain output at home.
- Compression garments: A compression garment or bandaging may be advised, particularly after groin dissection, to reduce swelling and the risk of lymphoedema.
Wound Care
- Dressings: Dressings should be kept clean and dry for the first 48 hours; gentle showering is usually permitted thereafter, taking care not to dislodge the drain.
- Cleaning: Gentle washing with mild soap and water is encouraged once dressings are removed, and wounds should be dried carefully.
- Activity: Gentle mobilisation is encouraged from the first day after surgery, with gradual return to normal activities over 4 to 6 weeks. Specific shoulder, arm or leg exercises will be advised to reduce stiffness and lymphoedema.
Scar and Lymphoedema Advice
- Scar Care Products: Silicone gels or sheets and regular moisturising once the wound has fully healed help optimise the final scar.
- Sun Protection: Protect the scar from direct sun exposure for the first 6–8 weeks to minimise pigmentation changes.
- Lymphoedema prevention: You will be advised on limb elevation, skin care, avoidance of injury and when to seek early specialist lymphoedema assessment.
Follow-Up
- Initial Post-Op Visit: A wound and drain check is typically arranged within the first week after discharge, often by a specialist nurse, to monitor drain output and decide when it can be removed.
- Histology & MDT: All removed nodes are examined in detail; results are discussed at the skin cancer multidisciplinary team meeting and shared with you, usually within 2 to 3 weeks of surgery.
- Adjuvant Treatment: Where appropriate, referral for adjuvant immunotherapy, targeted therapy or radiotherapy is arranged based on the MDT discussion.
- Surveillance: Structured follow-up is organised in line with national guidelines, including regular clinical examinations and, where indicated, surveillance imaging for several years.
- Lymphoedema Service: Prompt referral to a specialist lymphoedema service is arranged if swelling develops, to provide timely treatment and long-term support.
- Long-Term Care: Mr Singh remains available for any concerns or further follow-up as required throughout your surveillance period and beyond.
Procedure Summary
Ready to Discuss Lymph Node Dissection?
If you have been advised that lymph node dissection may be necessary as part of your skin cancer treatment, please feel free to contact us to answer any questions you may have or to schedule a consultation with Mr Singh.
Book a Consultation