Skin Cancer Surgery
As a plastic surgeon with a specialist interest in skin oncology, Mr Singh provides the full range of surgical treatments for skin cancers including basal cell carcinoma (BCC), squamous cell carcinoma (SCC) and melanoma. Treatment is tailored to the type, size and location of the tumour and includes wide local excision and, where required, reconstruction with local flaps or skin grafts.
Overview
Skin cancer is the most common cancer in the UK and encompasses a wide spectrum of disease, ranging from slow-growing, locally destructive tumours to aggressive lesions with the potential to spread. Early diagnosis and appropriate surgical treatment offer the best chance of cure for most skin cancers. Mr Singh works closely with dermatology, oncology and radiology colleagues as part of a specialist skin cancer multidisciplinary team to ensure each patient receives the most appropriate treatment plan.
Basal Cell Carcinoma (BCC)
BCC is the most common form of skin cancer and typically arises on sun-exposed areas such as the face, scalp, ears, neck and back. It grows slowly and very rarely spreads to other parts of the body, but can cause significant local tissue destruction if left untreated. Surgical excision with an appropriate margin of healthy tissue is the gold standard treatment for most BCCs.
Squamous Cell Carcinoma (SCC)
SCC is the second most common skin cancer and arises from the keratinocytes of the epidermis, often on sun-exposed sites. Unlike BCC, SCC has a small but real potential to spread to local lymph nodes or further afield, particularly when large, deeply invasive or poorly differentiated. Wide local excision with clear margins is the mainstay of treatment and some patients may need additional investigations or treatment to the regional lymph nodes.
Melanoma
Melanoma arises from the melanocytes (pigment-producing cells) of the skin and can behave aggressively with a significant potential to spread. It is the skin cancer most responsible for skin-cancer-related mortality. Initial treatment involves excision biopsy of the suspicious lesion, followed, once the diagnosis and thickness (Breslow depth) are confirmed on histology, by a wider local excision with defined margins based on national guidelines. In selected cases, sentinel lymph node biopsy is recommended for staging.
Benefits
- Curative treatment: Surgical excision offers the highest cure rates for most non-melanoma skin cancers and for early-stage melanoma.
- Histological confirmation: The specimen is carefully examined by a pathologist to confirm the diagnosis, assess margins and stage the disease.
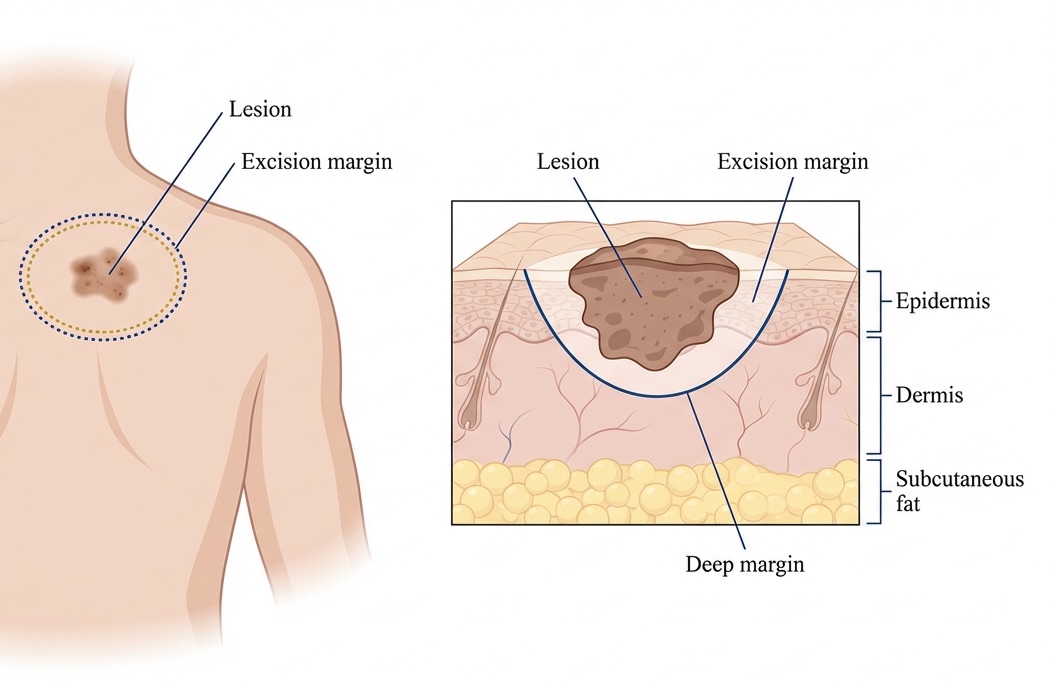
- Margin control: A defined margin of normal-appearing skin is excised around the tumour to reduce the risk of local recurrence.
- Immediate reconstruction: In most cases, the defect created by excision is closed or reconstructed in the same operation, restoring form and function.
- Specialist MDT care: Mr Singh participates in a skin cancer multidisciplinary team to ensure your care is planned and reviewed with other specialists.
- Tailored approach: The surgical plan is individualised to the tumour type, size, location and your overall health.
Surgical Techniques
The surgical approach depends on the type of cancer, its size and location, and the need for reconstruction. Mr Singh will discuss the recommended plan with you during your consultation.
- Excision biopsy: For suspected melanoma the entire lesion is usually removed with a narrow 2mm margin to enable the pathologist to determine the diagnosis and Breslow thickness.
- Wide local excision: The tumour is removed with a predefined margin of clinically normal skin, typically 4mm for BCC, 4–6mm for SCC and 1–2cm for melanoma depending on Breslow thickness, in accordance with national guidelines. The depth of excision is also tailored to the tumour.
- Primary closure: Where the defect is small, the wound edges can be brought together directly with sutures to achieve a fine linear scar.
- Local flap reconstruction: When a simple closure would distort surrounding structures (particularly on the face), a local flap of adjacent skin and soft tissue is mobilised to fill the defect whilst preserving function and appearance.
- Skin grafting: For larger defects, a split-thickness or full-thickness skin graft may be harvested from another part of the body and inset into the wound.
- Margin assessment: The excised specimen is carefully orientated and sent for histological examination; if any margin is found to be involved, further surgery may be required.
Risks & Considerations
General Risks
- Infection: Wound infection may occur and can delay healing or require antibiotics.
- Bleeding: Bleeding or haematoma formation can occasionally require further intervention.
- Scarring: A permanent scar is inevitable. Mr Singh will plan incisions to fall in natural skin creases or lines of relaxed skin tension where possible.
- Anaesthetic risks: Where general anaesthesia is used, standard anaesthetic risks apply.
Specific Risks to Skin Cancer Surgery
- Incomplete excision: Despite careful planning, histology can show tumour at or close to the margin, requiring further surgery.
- Local recurrence: Even after apparently complete excision, the cancer can rarely recur at the same site and requires ongoing surveillance.
- Nerve injury: Particularly on the face, small sensory or motor nerves may be affected, leading to numbness or, rarely, temporary or permanent weakness.
- Flap or graft complications: Partial or full loss of a flap or skin graft can occur, delaying healing and occasionally requiring revision surgery.
- Contour deformity: Removal of larger tumours can leave a visible depression, asymmetry or distortion of nearby structures such as the eyelid, lip or nostril.
- New skin cancers: Patients who have had one skin cancer are at increased risk of developing further skin cancers and require ongoing skin surveillance.
Recovery
Wound Care
- Dressings: Dressings vary depending on the reconstruction; local flap dressings are usually kept dry for 48 hours whilst skin grafts often require a bolster dressing which stays in place for 5 to 7 days.
- Cleaning: Once dressings are removed, gentle cleaning with mild soap and water is encouraged and daily showering helps to keep the wound clean.
- Sutures: Facial sutures are typically removed at around 5 to 7 days; sutures elsewhere at 10 to 14 days. Deep sutures are usually absorbable.
- Activity: Light activities can usually be resumed within a few days, but vigorous exercise and heavy lifting should be avoided for 2 to 4 weeks depending on the size and site of surgery.
Scar Advice
- Scar Care Products: Silicone gels or sheets and regular moisturising help optimise the appearance of scars.
- Sun Protection: Sun protection is essential not only to improve scar appearance but also to reduce the risk of further skin cancers. Use a high factor sunscreen daily and avoid sunbeds.
- Massage: Once fully healed, gentle scar massage can help soften and flatten the scar.
Follow-Up
- Initial Post-Op Visit: Typically scheduled around a week following surgery to check wound healing and remove sutures if needed.
- Histology & MDT: Results are discussed at a specialist skin cancer multidisciplinary team meeting. You will be contacted with the result and any recommended next steps, usually within 2 to 3 weeks.
- Surveillance: Formal follow-up in a skin cancer clinic is arranged in line with national guidance, with the interval and duration depending on the type and stage of the cancer.
- Self-Examination: You will be advised on how to examine your skin and lymph node areas regularly and when to seek urgent review.
- Long-Term Care: Mr Singh remains available for any concerns or further follow-up as required throughout your surveillance period and beyond.
Procedure Summary
Ready to Discuss Skin Cancer Treatment?
If you have a suspicious skin lesion or have been diagnosed with a skin cancer, please feel free to contact us to answer any questions you may have or to schedule a consultation with Mr Singh for specialist assessment and treatment.
Book a Consultation